Jun 22, 2022
By Jon Kelvey
The technique for giving medications by syringe is fairly straightforward. You have to invert the medicine vial to avoid drawing air bubbles into the syringe. Hayley Arceneaux, a physician assistant at St. Jude Children’s Research Hospital in Memphis, Tennessee, knows that.
What she didn’t anticipate was how different things would be in microgravity.
As the medical officer aboard the SpaceX Inspiration4 mission last September—the first all-civilian orbital mission—it fell to Arceneaux to treat her crewmates nauseated by space adaptation syndrome inside the Dragon spacecraft. “The air bubbles kept floating all around, and you’re trying to chase this medicine down to draw it up,” she says. Not to mention maintaining the “proper positioning so that your patient isn’t floating while you’re trying to administer meds.”
Arceneaux isn’t a space medicine specialist (she works in pediatric oncology), but her SpaceX flight might well go down as an important inflection point in space medicine history. For starters, none of the crew were professional astronauts. They represent a new kind of space traveler: the civilian space tourist.
Arceneaux and her crewmates conducted a series of space medicine experiments, including blood draws, saliva swabs, and ultrasound imaging of various organs, providing data on themselves and on how well they could operate the equipment. The results of those experiments could help keep future astronauts—from NASA, private companies, and space agencies worldwide—healthy as they venture far from home.
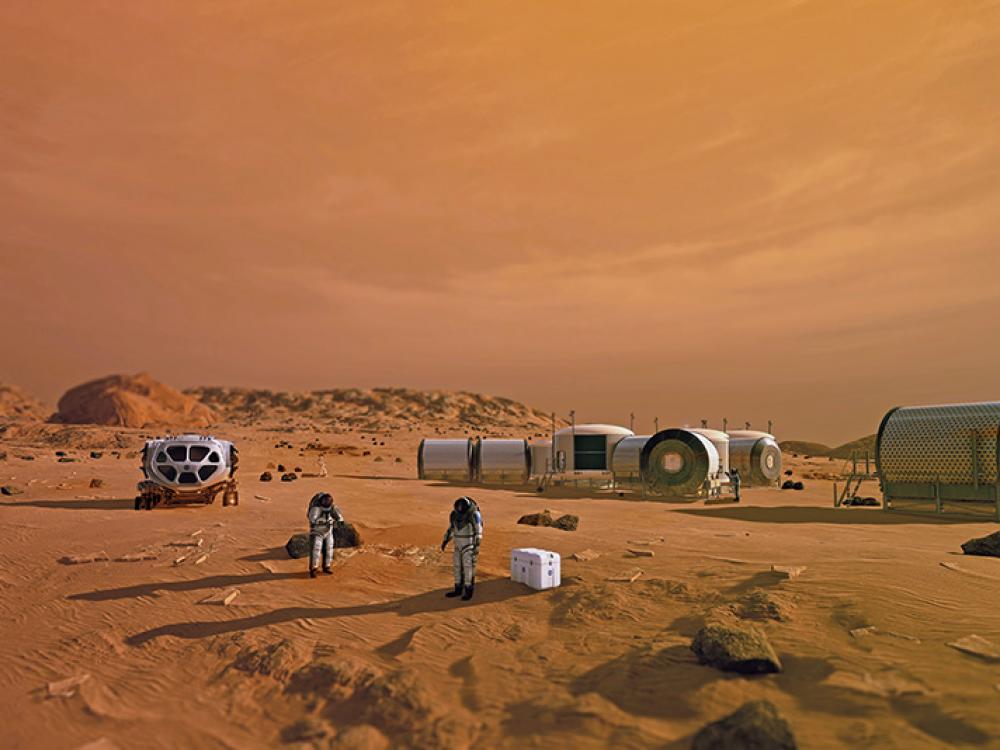
Consider a mission to Mars. It’s a roughly three-year deal, with six to nine months travel each way and a 40-minute roundtrip delay in communications with Earth during much of it. Unlike every human space mission to date, astronauts headed to Mars won’t be able to call up mission control and get expert advice quickly when they have a medical problem. They’ll have to deal with any emergencies on their own, with a very limited set of tools, medications, and expertise.

The U.S. Air Force was an early pioneer of space medicine: In 1949, a researcher tested a prone-position pilot’s bed, designed to relieve gravitational stress.
“Say you’re two weeks on your trip and you have a medical emergency,” says Emmanuel Urquieta, the chief medical officer for the Translational Research Institute for Space Health (TRISH) at Baylor College of Medicine in Houston, Texas. “You cannot just go 180 [degrees] and come back.” You have to go all the way to Mars and then return.
TRISH partners with NASA to develop space medicine solutions for the myriad hazards astronauts will face on such a mission: medical emergencies, muscle and bone loss due to long periods of microgravity, and the near-constant bath of cosmic radiation. Ensuring proposed solutions will work is much like the clinical trial process on Earth, and researchers need a lot of data. This is why TRISH funded some of the Inspiration4 experiments. It’s an opportunity for more data, and more diverse data, from four regular people flying in space.
“To be honest, going to space never crossed my mind,” says Arceneaux. “But also, it was never a possibility for me. I would not have made it through the NASA selection process because of the internal prosthesis in my leg.” As a child, she was successfully treated for bone cancer at St. Jude, leaving her with a titanium rod in her body and a passion for pediatric oncology. Arceneaux is the first pediatric cancer survivor and the first person with a limb prosthesis to fly in space—exactly the sort of person researchers would like to study.
After all, Arceneaux and her crewmates are historic anomalies. In 60 years of human spaceflight, around 600 people have flown in space. The vast majority of them have been hyper-fit white men with military experience.
It was 1971, and Apollo 15 astronauts David Scott and Jim Irwin were undertaking a grueling 18.5 hours of exploration over three days when a flight surgeon at mission control noticed something wrong with Irwin’s heart. If he had been on Earth, Irwin would have been on his way to the hospital. But given the 100-percent-oxygen environment and microgravity easing the stress on his heart, the surgeon concluded that, for the time being, Irwin was probably better off in space.
“I think that was kind of putting a happy face on a very tense moment,” says Jordan Bimm, a historian of space science and technology at the University of Chicago. The medical team at mission control kept a watch on Irwin the whole way home, praying he wouldn’t go into cardiac arrest and die in space. (He made it home safely, though he would pass away from a cardiac event in 1991.)
Irwin’s health scare in space was never supposed to happen. “This was not a problem that was caught in any of the screenings,” says Bimm. Space missions were “complex human-machine systems, and they knew right from the start that both the human and the machine had to function as advertised.” A whole lot of testing went into ensuring the machines could fly astronauts safely, and a whole lot of thought went into which astronauts could safely fly those machines. The Mercury Seven astronauts were ultimately selected from the elite of the military test pilot corps for just this reason—a cautious choice that Bimm notes set a precedent in astronaut selection that took a long time to overturn.
Irwin’s close call aside, no American astronauts have perished in space. But as spaceflights grew longer, so did the list of potential ailments even very fit astronauts could not ignore.
The lesson, Bimm says, and as Arceneaux learned firsthand, is that space is a new normal. “We calibrate so much of our medical knowledge and practices to Earth normal, and only so much of that is transferable to microgravity,” says Bimm. A similar dynamic might exist between space medicine solutions developed for the International Space Station (ISS) and missions venturing beyond Earth’s orbit. There’s Earth normal, ISS normal, and then there’s deep space and Mars normal.
When I connect with Kerry Lee over video conference, he apologizes for the noise. Rather than speaking to me from home, he was in a back room at the “office”—mission control at Johnson Space Center in Houston. “We had an energetic solar particle event occur since we set this up,” he says, sporadic updates buzzing over the intercom. “It’s an interesting time because we haven’t had one in four years, so you may hear some stuff in the background.”
As the operations lead for NASA’s Space Radiation Analysis Group, Lee is charged with keeping ISS astronauts safe from space radiation. When he and his team get word of a Solar Particle Event (a stream of highly energetic charged particles accelerated by energy released from our star), they immediately plot the location of the space station. “It turns out for this particular event, they’re well protected by the Earth’s magnetic field,” says Lee. The shields are always up around starship Earth, our planet’s magnetosphere deflecting solar particles and some higher energy galactic cosmic rays. But astronauts venturing to the moon and beyond can’t take that magnetic shield with them.
To combat radiation from solar storms, future astronauts can make use of lessons learned on the International Space Station, according to Lee, who is also the radiation system manager for NASA’s Orion vehicle, which is slated to ferry NASA astronauts back to the moon in 2025. While plastic (high density polyethylene) is a desirable material to use, the Orion vehicle does not have the luxury of carrying mass that only serves a single purpose, so it uses stowage that is already on board as shelter from radiation. (Lead is great for blocking X-rays at the dentist, but it will generate dangerous secondary radiation when struck by the protons that constitute most space radiation.)
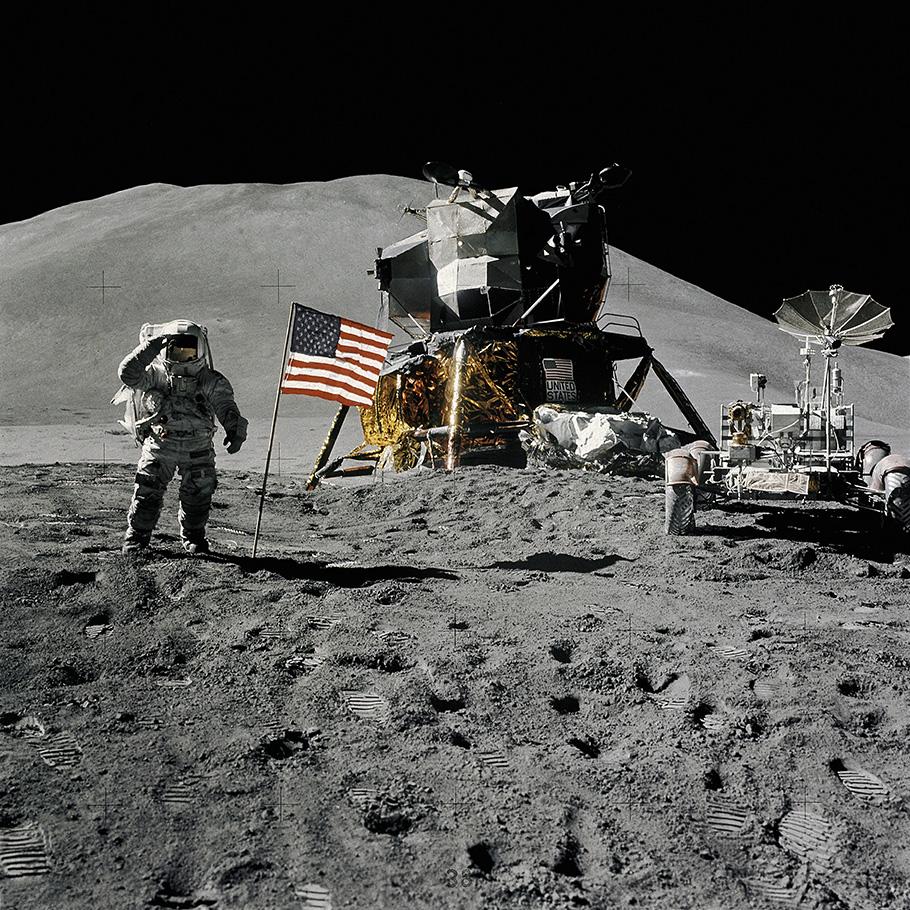
As Apollo 15 astronauts David Scott and Jim Irwin explored the moon, mission control noticed that Irwin was experiencing irregular heart rhythms.
Unfortunately, higher energy galactic cosmic rays are another matter. “The mean energy of a galactic cosmic ray proton can pass through like a meter of material,” says Lee. Exposure to cosmic radiation then becomes a calculated risk for deep-space astronauts. There are some advanced concepts under consideration at NASA, Lee says, such as large electrostatic screens to intercept cosmic rays, but for now they remain only concepts. “I think the money is probably better spent in developing propulsion,” he says. Fly faster, absorb less radiation.
Apollo 15 astronaut James Irwin.
Radiation isn’t the only threat, of course. There’s also space itself: a ruthless, cold vacuum. “At the end of the day, I think, there just needs to be a real good, healthy respect that space is not conducive to life,” says TRISH senior biomedical engineer Jimmy Wu, who spends a lot of time thinking about this stuff. “It will kill you.”
Then there are altered gravity fields, the space medicine catchall for everything from zero gravity to the one-third of Earth’s gravity astronauts would experience on Mars. In addition to causing things like blood clots and kidney stones, microgravity can wither bones and muscle to the extent that astronauts would need help walking after a long stint away from terra firma.
The challenges of long-distance space travel aren’t just physiological: Future astronauts will need to cope with extended isolation and confinement. A Mars crew needs to work well together for long stretches, and three years is a long time to spend with the same three people, living together in what are essentially pressurized cans. Compounding the psychological challenges is the distance from Earth. “You cannot say, ‘Houston, we have a problem,’ ” says Urquieta. “That message is going to take 20 minutes and then another 20 for Houston to say ‘Okay, what’s the problem?’ ”
One lesson from space travel that also applies to medicine, Wu says, is that you want to avoid flying the newest technology, as it’s not yet proven to be robust in extreme environments like space. But you also need to keep pushing the edge of what’s possible. TRISH funds the entire spectrum. On the one hand, the University of Pittsburgh is developing human hibernation technology. On the other, TRISH funded the Butterfly iQ+ultrasound experiment on Inspiration4, a miniaturized ultrasound device paired with a smartphone as an interface. Miniaturization, in general, would solve a lot of problems. For instance, NASA’s Glenn Research Center is researching a streamlined version of the bulky exercise equipment used aboard the space station to fit inside the Orion spacecraft.

The civilian crew of the SpaceX Inspiration4 mission (standing in front of their Falcon 9 and Dragon spacecraft) conducted a series of medical experiments in orbit. (Flickr/Inspiration4/John Kraus)
But some space medical challenges require technology that is still out-of-reach. Take medicines: Whether it’s drugs to treat space adaptation syndrome (vomiting is no fun for anyone involved), depression due to isolation, blood clots, even cancer, a Mars mission needs to carry everything the crew might need. But there’s not room for everything.
“The example we use here a lot is intravenous (IV) fluid,” says Kris Lehnhardt, a physician and lead scientist for exploration medical capability in NASA’s Human Research Program. If you run out of IV fluids halfway through the mission (maybe from treating kidney stones), there’s no resupply available. But every liter of IV fluid you take with you is a liter of something else you have to leave at home. So NASA is researching a two-birds, one-stone solution: turning potable water into IV fluid. Says Lehnhardt: “Give the IV fluid to astronauts, and then when they pee, you can recycle that pee into potable water and make more IV fluid.”
Because some medications would expire over the course of a three-year mission, Lynn Rothschild, a researcher at NASA Ames in California, is working on a project called Astropharmacy—funded by NASA’s innovative advanced concepts program—that could help with the constraints of both space and time. If you genetically engineer bacteria to produce protein-based medications known as biologics, you can save the dehydrated spores on substances that might include paper. Need a drug? Use a hole punch and “activate it by giving it the culture medium, and they should start pumping proteins out of the cell,” says Rothschild. The result is a profusion of drugs made on-demand, and with minimum space requirements. “I’m aiming for something that’s the size of a wallet,” says Rothschild—or maybe a credit card.
But even with a drugstore the size of a credit card, you still can’t take it all with you. “When you have to decide what you take, and you know you can’t take everything you want, how do you make those decisions?” asks Lehnhardt.

Last September, Hayley Arceneaux became the first pediatric cancer survivor and the first person with a prosthetic limb to fly in space. (Flickr/Inspiration4 Crew)
Mission planners are trying to predict the most likely—and the most likely of unlikely—medical problems a deep-space crew might face. “They call it the integrated medical model,” says Urquieta, a list generated by millions of computer cycles using repeated random samplings. The list contains everything from a bad headache to massive blood loss, but “when you put the list next to conditions that have actually happened in space, the conditions that have actually happened are the really minor ones,” he says, like losing a fingernail. “In the 20 years plus of the International Space Station, there haven’t been any major medical emergencies.”

Astronauts aboard the International Space Station conduct research on fluid shifts in the body, which can affect the brain and vision.
That isn’t as reassuring as it sounds, given it’s based on ISS normal. What’s Mars normal like?
Mars, Lehnhardt notes, is roughly 1,000 times further from the moon than the moon is from Earth, and the moon is 1,000 times further from Earth than is the space station. The moon’s gravity is one-sixth of Earth’s, closer to the one-third G of Mars than the microgravity on the ISS. That makes the moon an ideal stepping stone. “If Mars is the marathon, then the moon is like a 5K,” says Lehnhardt. “We are going to be spending weeks to months in lunar orbit and on the lunar surface, and we are going to be testing and developing and simulating all of those Mars operations from a medical perspective.” This upcoming lunar research might study how astronauts’ bodies respond to long periods in low gravity. And it will involve increasingly Mars-like operations, for which astronauts perform complex activities with simulated Mars mission communications delays, Lehnhardt says.

Inspiration4 crew members examine themselves with a Butterfly iQ+ultrasound. (Flickr/Inspiration4 Crew)
Fifty years ago, the Apollo astronauts had limited medical training and relied on an Earth-based flight surgeon for medical issues. In a NASA report, one unnamed Apollo astronaut expressed his desire for onsite medical care: “Hell, if they can take a naval aviator and train him to do geology [on the moon], they sure as hell can train a doctor to do useful things.”
To that end, the Artemis lunar missions will likely test technology that relies on specialized software that guided ISS astronauts through kidney and bladder ultrasound procedures. Ultimately, NASA would like to have a medical decision support system, a computer that can guide a Mars crew through most medical procedures they might require—any member of the crew, for that matter. “If you follow Murphy’s law,” says Lehnhardt, then the crew medical officer is “going to become the person who becomes sick or injured.”
Jon Kelvey is a science writer covering space, aerospace, and biosciences.

The Apollo 11 command module medical kit had injectors for motion sickness and pain suppression.
Never leave Earth without a decongestant pill.
The National Air and Space Museum is home to an extensive collection of objects from NASA’s Apollo program, including Neil Armstrong’s spacesuit and the command module Columbia. But one of the most significant artifacts is something most of us would barely glance at: a bio-harness that flew aboard Apollo 11 to monitor an astronaut’s physiological functions.
When initial space mission planning began in 1959, equipment capable of transmitting biomedical data from space did not even exist. NASA brought together engineers and medical staff to develop the technology so that, when the first astronauts blasted off from Earth during the Mercury program (1961-63), they were wearing electrodes to collect electrocardiograms, a heated thermistor to detect breathing, and a rectal probe that recorded highly accurate body temperature readings. (Fortunately, for the Apollo astronauts, NASA concluded that temperature monitoring via rectum was not ideal for the lengthy journey to the moon and back.)

The Apollo 11 lunar module medical kit included pills and minor first-aid supplies.
Other crucial medical supplies can be found in the Museum’s collection, such as medical and first aid kits that went into space. The rudimentary medical kit used by the Mercury astronauts included autoinjectors—each one was fitted with a red safety cap that, when removed, armed a needle that could deliver a single dose of medication through the two-ply aluminum pressure-suit without causing a significant leak. During the initial four missions, these drugs included a stimulant, a painkiller, an anti-motion-sickness drug, and a vaso¬constrictor for treatment of shock.
The astronauts who flew on the Apollo missions required much more than the astronauts of the Mercury and Gemini programs. Two medical kits flew aboard each Apollo mission: one for the command module and one in the lunar module. The kits had expanded to include 30 different types of drugs over the course of Apollo. That pharmacy was put to good use as the astronauts endured a series of ailments during their time in space: dermatitis, insomnia, constipation, stuffy noses, upper respiratory infections, and sore throats.
Mark Strauss is the managing editor at Air & Space Quarterly.

We rely on the generous support of donors, sponsors, members, and other benefactors to share the history and impact of aviation and spaceflight, educate the public, and inspire future generations. With your help, we can continue to preserve and safeguard the world’s most comprehensive collection of artifacts representing the great achievements of flight and space exploration.
We rely on the generous support of donors, sponsors, members, and other benefactors to share the history and impact of aviation and spaceflight, educate the public, and inspire future generations. With your help, we can continue to preserve and safeguard the world’s most comprehensive collection of artifacts representing the great achievements of flight and space exploration.






